SCOPE
What is SCOPE?
Safer Care for Older Persons (in residential) Environments (SCOPE) took place from September 2018 to April 2019 as a randomized controlled trial examining the effect of a quality improvement (QI) intervention that empowered health care aides to take the lead on improvement strategies within their nursing home. SCOPE also aimed to improve the quality of work life for staff, demonstrated by measures of work engagement, staff empowerment and job satisfaction.
SCOPE placed special emphasis on developing the leadership skills of care aides and senior leadership for successful operation. This was achieved by providing additional training/coaching for facility management on how to support the frontline teams to succeed with their improvement strategies.
By empowering frontline staff such as care aides, SCOPE aimed to increase the use of best practices among frontline staff, thereby leading to improved quality of care for residents.
What was involved?
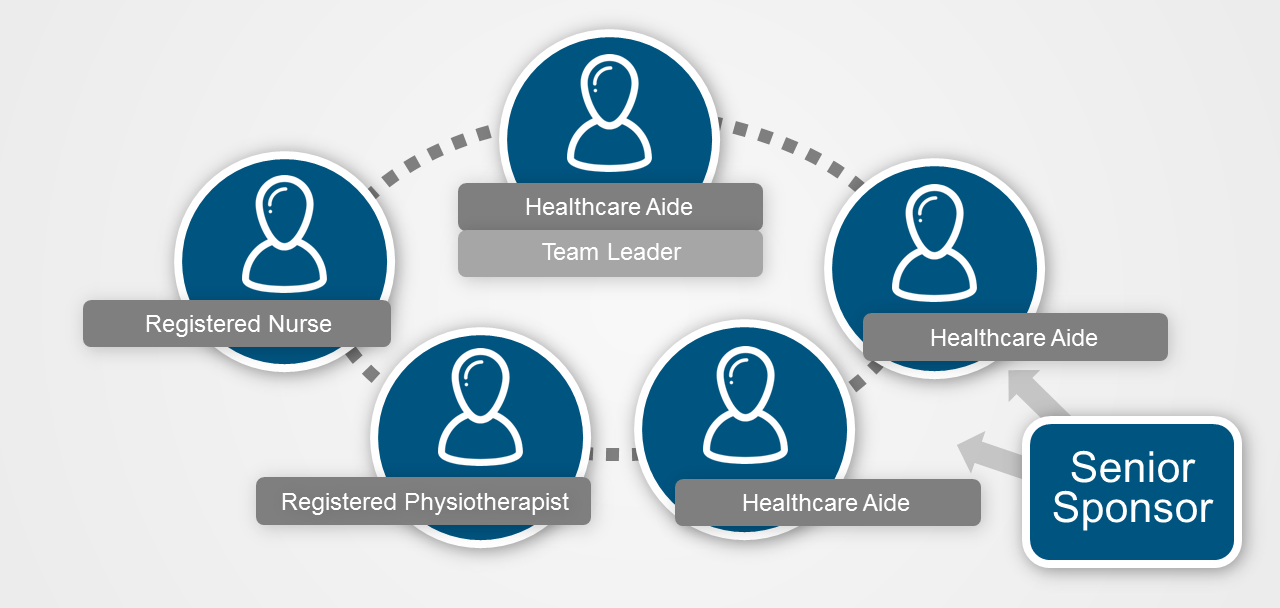
Teams of five staff members on one unit within a participating nursing home initiated and tested the effect of quality improvement activities in their daily delivery of care. The teams were made up of 3 care aides (one of whom led the team) and 2 other members of staff, with support from a Team Sponsor and a Senior Sponsor. Each team chose to focus on one of three areas: recognizing and treating pain, optimizing resident mobility or accommodating dementia-related responsive behaviour.
Throughout the year that the intervention took place, teams received regular coaching from the SCOPE Quality Advisor and participated in monthly teleconferences. They also attended four Learning Congresses - events that brought together all teams to participate in educational sessions, and share their challenges.
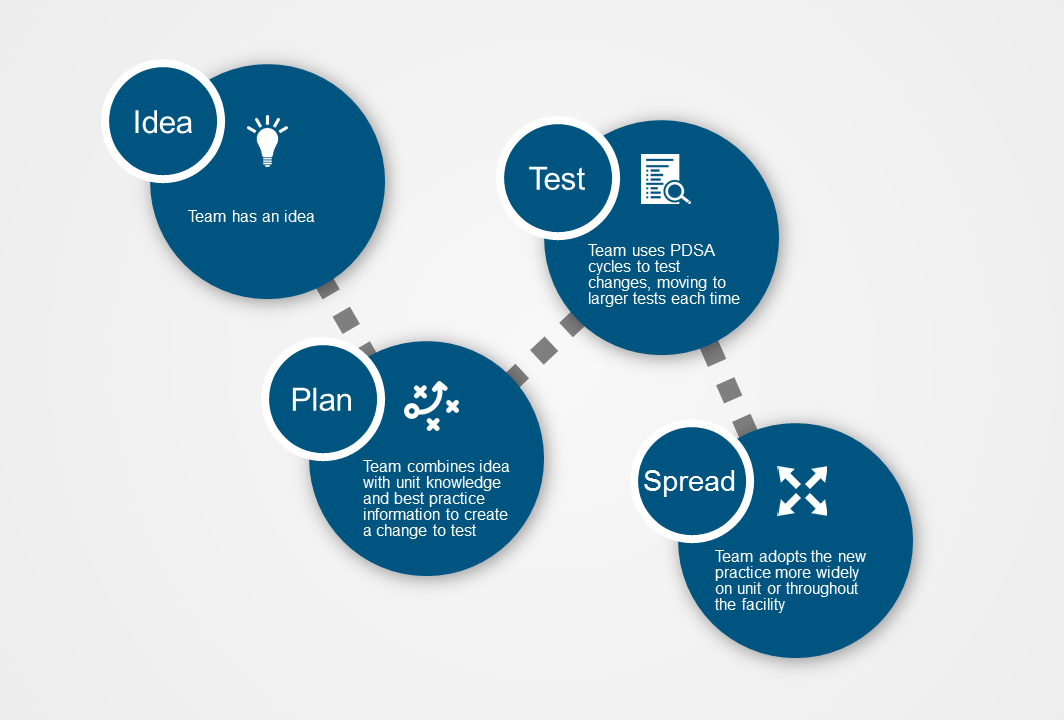
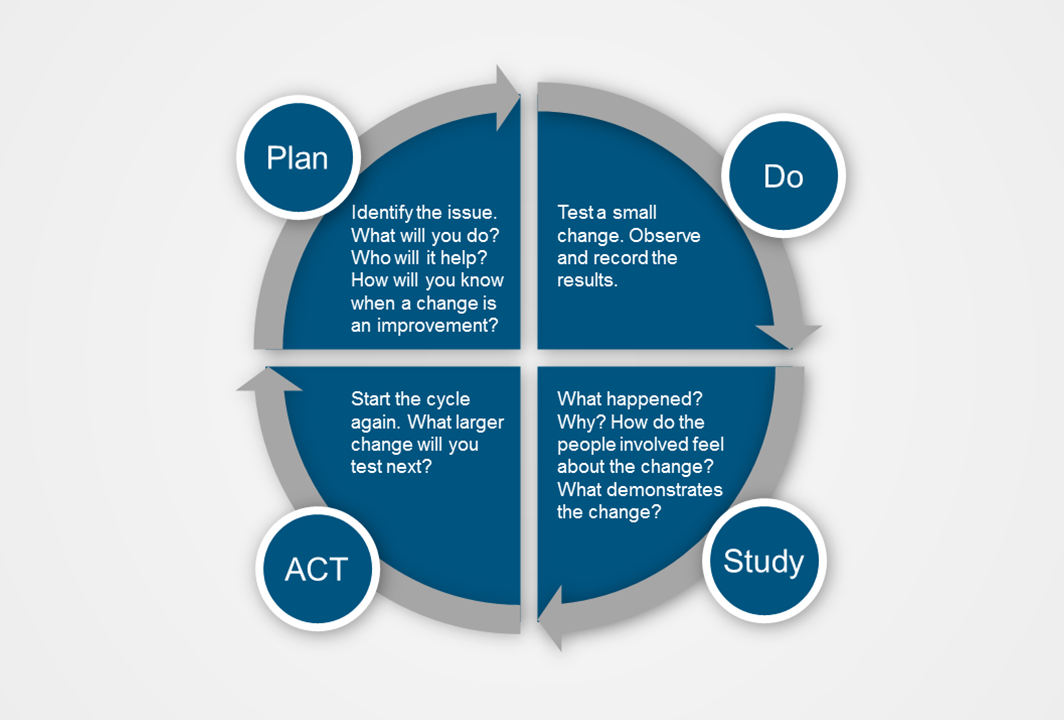
At each Learning Congress, teams learned about the principles of Quality Improvement, how to conduct Plan-Do-Study-Act cycles, how to collect information and measure the effects of their changes and how to adapt, adopt or abandon their changes based upon their results. All of this happened while teams created, practiced and adapted change ideas to improve the lives of their residents and also engaged the clinical teams on their units.
At the final Learning Congress, each team shared their journey through SCOPE, presenting stories of both success and failure. Care aides talked about how SCOPE had empowered them to make these changes, had given them a greater sense of worth and had changed them, their way of looking at residents and allowed them to adopt new ways of doing.
Additionally, via the SCOPE Leadership Stream, senior sponsors and team sponsors came together on a monthly basis and at each Congress, to receive coaching on how to support the teams.
Quality Improvement Team
What were the benefits?
- An opportunity to improve care in an area selected by the team
- Staff learning and development in the area of quality
- Increased staff engagement and mobilization of their experiential (tacit) knowledge
- Acquisition of a method that can be used to tackle other quality areas in the future
- Potential for the spread of improvement methodology throughout the facility
- Participation in Learning Congresses
- Sessions on leadership for senior facility staff
How did we measure success?
Baseline data for each facility involved in SCOPE were collected via the TREC Measurement System (TMS). This data collection was repeated 4-6 months following the final Learning Congress to look for any changes. During the intervention, one of the key ways success in SCOPE was measured was with control charts.
Control charts (run charts) enable the mapping of resident outcomes (e.g., a quality indicator or a scale) over time and determine if observed improvements are “real” or part of the normal variation seen in clinical settings. Teams were taught how to record data and construct these charts by the Quality Advisors, so that they could see what was changing in ‘real time.’
Why is SCOPE important?
Nursing home residents are among the most vulnerable population in Canada. The demand for residential care for older persons with complex needs will only continue to increase. Quality of care and quality of life will remain a major challenge.
Our original SCOPE pilot in Manitoba (2010-2012) showed that, with support, care aides can successfully lead local quality improvement initiatives resulting in improved resident outcomes and increased work engagement. Our full scale evaluation of the SCOPE model assessed its success across a wider range of settings, building on findings from the pilot about how to implement the model.
Publications
Nooraie, R.Y., Qin, Q., Wagg, A., Berta, W., and Estabrooks, C.A. (2024). Building a communication and support network among quality improvement teams in nursing homes: a longitudinal study of the SCOPE trial. Implementation Science Communications, 5(1):19.
Wagg, A., Hoben, M., Ginsburg, L., Doupe, M., Berta, W., Song, Y., Norton, P., Knopp-Sihota, J., & Estabrooks, C. A. (2023). Safer Care for Older Persons in (residential) Environments (SCOPE): a pragmatic controlled trial of a care aide-led quality improvement intervention. Implementation Science. 18(1): 1-14.
Song, Y., MacEachern, L., Doupe, M.B., Ginsburg, L., Chamberlain, S.A., Cranley, L., Easterbrook, A., Hoben, M., Knopp-Sihota, J., Reid, R.C., Wagg, A., Estabrooks, C.A., Keefe, J.M., Rappon, T., & Berta, W.B. (2022). Influences of post-implementation factors on the sustainability, sustainment, and intra-organizational spread of complex interventions. BMC Health Services Research 22(1):666.
Doupe, M., Brunkert, T., Wagg, A., Ginsburg, L., Norton, P. Berta, W., Knopp-Sihota, J., & Estabrooks, C.A. (2022). SCOPE: Safer care for older persons (in residential) environments: a pilot study to enhance care aide-led quality improvement in nursing homes. Pilot and Feasibility Studies, 8(1):26.
Cranley LA, Hoben M, Yeung J, Estabrooks CA, Norton PG, Wagg AS. (2018). SCOPEOUT: Sustainability and spread of quality improvement activities in long-term care: A mixed methods approach. BMC Health Services Research, 18:171.
Norton PG, Cranley LA, Cummings GG, Estabrooks CA. (2013). Report of a pilot study of quality improvement in nursing homes led by healthcare aides. European Journal for Person Centered Healthcare, 1(1), 255-264.
Cranley LA, Norton PG, Cummings GG, Barnard D, Estabrooks CA. (2011). SCOPE: Safer Care for Older Persons (in residential) Environments – A study protocol. Implementation Science, 6:71.
Page Options


